| Date | May 2017 | Marks available | 4 | Reference code | 17M.3.SL.TZ2.22 |
| Level | Standard level | Paper | Paper 3 | Time zone | Time zone 2 |
| Command term | Explain | Question number | 22 | Adapted from | N/A |
Question
Explain a method to quantify the energy content in food.
Markscheme
a. description of apparatus
OR
drawing
OR
measured with a calorimeter
Allow other correct described method.
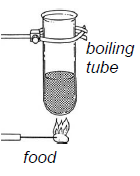
b. measure the initial mass/volume of water
c. measure the initial temperature of the water
d. measure the mass of the food
e. ignite the food and place under the container of water
f. measure the final temperature of the water
OR
calculate the change in temperature of the water
g. heat gained by the water=heat lost by the food
OR
energy=mass of water temperature rise in water x specific heat capacity of water/mass of food
| Date | May 2017 | Marks available | 1 | Reference code | 17M.3.SL.TZ1.17 |
| Level | Standard level | Paper | Paper 3 | Time zone | Time zone 1 |
| Command term | Outline | Question number | 17 | Adapted from | N/A |
Question
Breastfed infants with rickets sometimes have seizures due to low blood calcium levels. A study was carried out to investigate the relationship between maternal blood vitamin D levels and the incidence of these infant seizures.
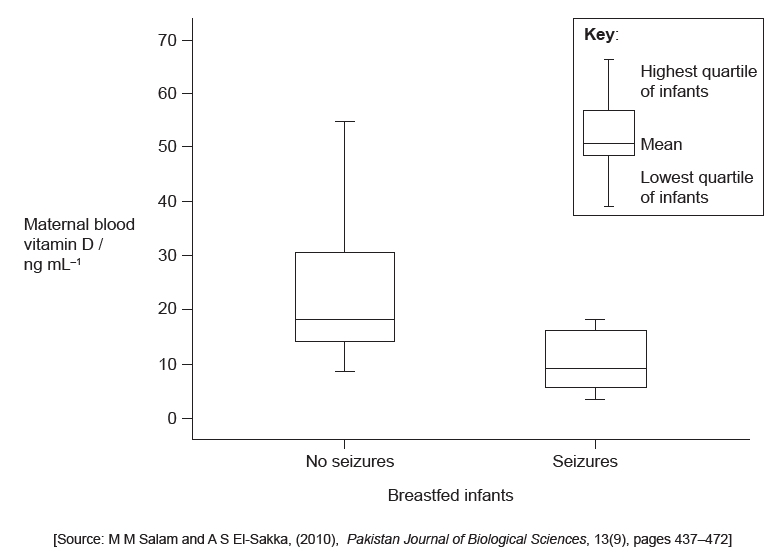
Describe the relationship between the maternal blood vitamin D levels and the incidence of seizures.
Deduce the reason for rickets in these infants.
Identify the reason for vitamin D not being considered to be a typical vitamin.
Outline the reason for some amino acids being classified as essential amino acids.
Markscheme
infants from mothers with low levels of vitamin D have an increased chance of developing seizures
Accept answers in the converse.
lack of vitamin D in breast milk OR lack of vitamin D leads to lack of bone mineralization/calcium uptake
it can be synthesized by humans «in skin»
a. they cannot be synthesized by humans
b. they must be present in the diet
| Date | November 2016 | Marks available | 2 | Reference code | 16N.3.SL.TZ0.17 |
| Level | Standard level | Paper | Paper 3 | Time zone | TZ0 |
| Command term | Suggest | Question number | 17 | Adapted from | N/A |
Question
The table shows the nutritional information for two different types of milk as it is displayed on the carton. The information in both tables is based on a 250 g serving and shows the recommended daily allowance (RDA) for each nutrient.
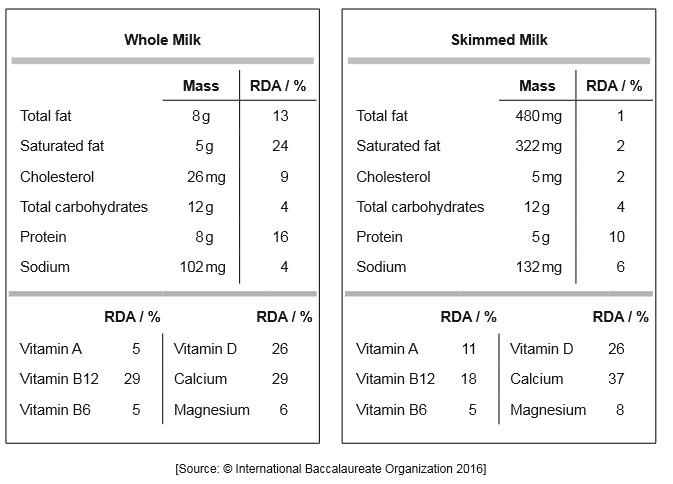
Calculate how many grams of protein should be consumed each day. Working is not required.

State one function of sodium in the diet.
Identify, with a reason, which milk provides more energy in a 250 g serving.
Suggest, with reasons, which milk would be recommended for someone with osteomalacia.
Markscheme
50 «g»
water balance/osmoregulation/transmit impulses along nerves/muscle contraction/blood pressure/ sodium potassium pump/sodium-glucose cotransporter / sodium-amino acid cotransporter
whole milk because it contains more fat/energy
Reason is required.
a. skimmed milk has more calcium so better
b. both milks have the same amount of vitamin D so no difference between the two.
Skimmed milk alone is worth no marks. Two reasons are required for both marks.
| Date | November 2016 | Marks available | 3 | Reference code | 16N.3.SL.TZ0.16 |
| Level | Standard level | Paper | Paper 3 | Time zone | TZ0 |
| Command term | Explain | Question number | 16 | Adapted from | N/A |
Question
A study undertaken in West Virginia, USA, shows the relationship between body mass and the probability of having hypertension or type II diabetes. The test subjects in the study were classified as normal, overweight or obese according to their body mass index (BMI).
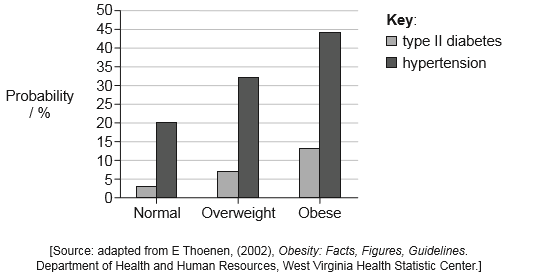
Identify the increased probability of an obese person having hypertension relative to someone who has normal weight.
Explain how the administration of a drug that stimulates the leptin receptors in the hypothalamus could help treat obesity.
Markscheme
24%
a. appetite control (centre) is located in the hypothalamus
b. leptin is a hormone made by fat/adipose cells
c. to inhibit appetite/feeling of hunger
OR
promotes feeling of satiety/fullness
d. the drug mimics the action of leptin
e. (reduced hunger) leads to less food intake/weight loss
| Date | May 2016 | Marks available | 2 | Reference code | 16M.3.SL.TZ0.17 |
| Level | Standard level | Paper | Paper 3 | Time zone | TZ0 |
| Command term | State | Question number | 17 | Adapted from | N/A |
Question
Numerous health benefits are associated with diets that include omega-6 fatty acids and omega-3 fatty acids in a ratio between 1:1 and 4:1. When consumed in excess, omega-6 inhibits uptake of omega-3. Many people in developed countries eat large amounts of processed foods and oils, so they consume omega-6 fatty acids and omega-3 fatty acids at a ratio of between 10:1 and 25:1. Such high ratios are associated with many chronic diseases.
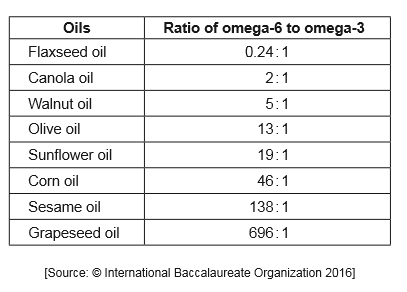
Deduce with reasons which two oils would be the best sources of fatty acids for a healthy diet.
Outline the meaning of the term essential when used to describe some fatty acids.
(i) State the name of the part of the brain where appetite is controlled.
(ii) State the role of the vagus nerve.
Markscheme
Canola AND flaxseed/walnut (Both needed)
Both have ratios within or close to recommended ratio
Fatty acids which have to be obtained in the diet
Fatty acids which cannot be synthesized in the body
(i) Hypothalamus (Do not accept appetite control centre)
(ii) Transmit impulses from brain to gland cells «in stomach»
Stimulate secretion by «stomach» gland cells
Stimulates secretion of gastric acid
Example of parasympathetic response eg: slows heart
Transmit sensory information to the brain
| Date | May 2015 | Marks available | 1 | Reference code | 15M.3.SL.TZ2.1 |
| Level | Standard level | Paper | Paper 3 | Time zone | Time zone 2 |
| Command term | Distinguish | Question number | 1 | Adapted from | N/A |
Question
Low protein diets are a widespread problem in the developing world. A low protein diet in a pregnant mother could affect a developing fetus. Other mammals are used as a biomedical model for energy metabolism and malnutrition in humans.
In an experiment to study the effect of protein levels in the diet, pregnant mammals were fed diets with different ratios of protein to carbohydrate:
• low protein : high carbohydrate (LP),
• adequate protein : adequate carbohydrate (AP),
• high protein : low carbohydrate (HP).
The table shows the average birth mass of the offspring and the body mass gain of the mother during the pregnancy. The concentration of several substances in the plasma of the mothers was also recorded. LDL (low density lipoprotein) is considered “bad cholesterol” and HDL (high density lipoprotein) is considered “good cholesterol”.
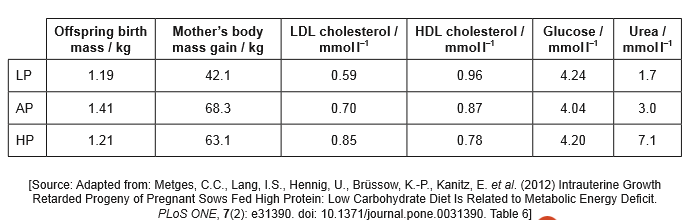
Identify the substance that varies the most in the plasma of the mothers.
Calculate the difference between birth mass of offspring whose mothers were fed the AP diet and the HP diet.
. . . . . . . . . . . . . . . . . . . . . kg
Distinguish between LDL cholesterol and HDL cholesterol in relation to the diet.
Explain the low birth mass of offspring born to mothers who were fed the LP diet.
In many societies doctors may recommend an HP diet for pregnant humans. Using the data, evaluate this recommendation.
Markscheme
urea
0.20 (kg) (less weight in HP)
LDL cholesterol increases and HDL cholesterol decreases as (proportion of) protein increases/carbohydrate decreases / OWTTE.
a. lack of essential amino acids to form protein;
b. not enough protein for growth;
c. not enough amino acids/protein to form muscle/tissues;
d. low protein may affect production of enzymes;
(the data does not support the recommendation):
a. as HP has the highest level of plasma urea which could be toxic;
b. HP has a high level of LDL/bad cholesterol and a low level of HDL/good cholesterol which could lead to coronary heart disease;
(accept high ratio of LDL: HDL)
c. HP produces a high level of glucose (compared to AP) which could lead to diabetes;
d. HP produces a low birth weight (compared to AP) which may affect development / OWTTE;
(the data does support the recommendation):
e. the mother has a similar weight gain to AP thus avoiding health problems;
| Date | November 2015 | Marks available | 1 | Reference code | 15N.3.SL.TZ0.1 |
| Level | Standard level | Paper | Paper 3 | Time zone | TZ0 |
| Command term | State | Question number | 1 | Adapted from | N/A |
Question
Nationally representative data was collected on body mass index (BMI) from 1985 to 2004.
The graph shows overweight and obesity patterns in adult males and females from seven countries.
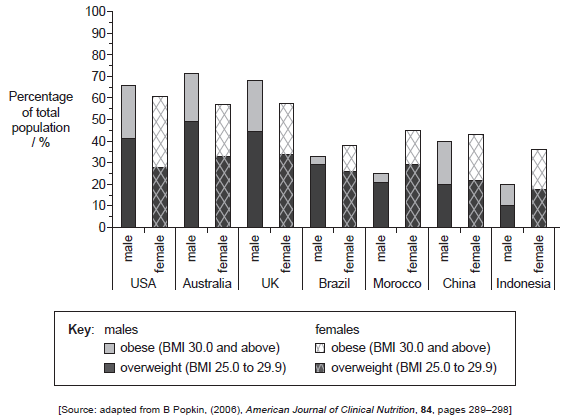
State which country has the lowest total percentage of overweight and obese adults.
Distinguish between the levels of male obesity and female obesity.
Compare the overweight and obesity patterns in Australia and Morocco.
Suggest two possible reasons for the differences in BMI from the reported countries.
Markscheme
Indonesia
a. higher percentage of obese females (compared to males);
b. greatest difference is in Morocco/Brazil;
c. least difference (between obese males and females) is in China/UK;
Accept numerical distinctions.
a. higher total percentage of overweight/obese in Australia (compared to Morocco);
b. Australia has more overweight/obese males than females and Morocco has more overweight/obese females than males / vice versa;
c. less difference between male and female obesity in Australia than Morocco / vice versa;
d. more overweight than obese in both Australia and Morocco;
a. different availability/poverty/costs of inexpensive high-energy/high fat/high sugar foods;
b. portion sizes / availability of away-from-home food/fast food;
c. different levels of activity / sedentary lifestyle;
d. cultural differences;
e. nutritional education;
f. genetic/inherited differences;
| Date | May 2013 | Marks available | 2 | Reference code | 13M.3.SL.TZ1.2 |
| Level | Standard level | Paper | Paper 3 | Time zone | Time zone 1 |
| Command term | Evaluate | Question number | 2 | Adapted from | N/A |
Question
The following are from the labels of a bag of all purpose white flour (wheat) and a bag of parboil long grain rice. Amounts shown are per serving.
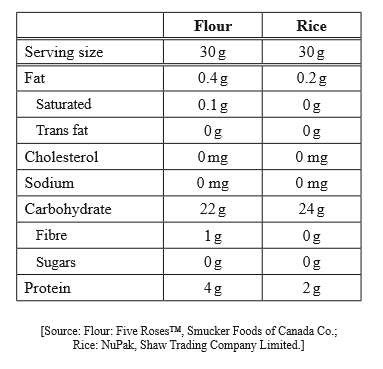
Using your knowledge of the energy content of nutrients, calculate the protein energy value of a serving of rice, showing the units.
Compare wheat flour and rice as main dietary sources of energy for humans.
Evaluate the benefits of reducing dietary cholesterol in lowering the risk of coronary heart disease.
Markscheme
a. energy value of 100 g protein ≈ 1720 kJ / energy value of protein ≈17 kJ/g;
b. 2g protein
energy value / ECF kJ of 100g protein
34.4 kJ/ECF kJ value;
100g protein
Answer range 34–35 kJ/ECF kJ.
For calculation note error carried forward.
Units required. If no units deduct a mark and indicate in scoris U –1.
a. wheat and rice almost equivalent for energy value;
b. rice has only slightly less kJ/energy from fat/protein / more from carbohydrate;
c. considering food miles / availability may be decision factor for choice;
a. dietary cholesterol correlated to blood cholesterol/fatty acids;
b. high blood cholesterol is an important risk factor (but not the only cause);
c. some cholesterol required for normal synthesis of body molecules;
d. genetic factors play an important role in determining cholesterol levels;
e. other environmental factors (smoking) play a role in determining cholesterol levels;
| Date | May 2013 | Marks available | 2 | Reference code | 13M.3.SL.TZ2.1 |
| Level | Standard level | Paper | Paper 3 | Time zone | Time zone 2 |
| Command term | Discuss | Question number | 1 | Adapted from | N/A |
Question
Malnutrition affects the body mass index (BMI) of mothers. The height and mass of over 7000 mothers in Ethiopia and the sex of their most recently born child was recorded. The graph shows the percentage of mothers with a BMI below 18.5 and the percentage of their most recent births that were males in 11 regions across Ethiopia.
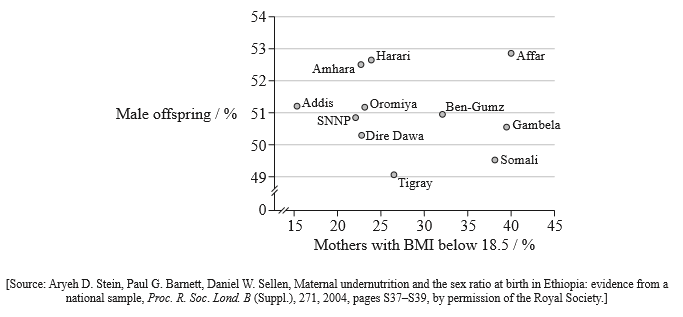
State the regions with the highest and lowest percentage of male offspring.
Region with highest percentage: ……………………………………………………………..
Region with lowest percentage: ……………………………………………………………..
Comment on the variation in BMI of mothers in Ethiopia.
Discuss whether the data supports the hypothesis that malnutrition affects the sex ratio of offspring.
Suggest one limitation of the data.
Suggest one factor that could cause malnutrition in mothers.
Markscheme
highest: Affar;
lowest: Tigray;
(both needed)
a. evidence of high malnutrition rates / some areas with many mothers below 18.5 BMI;
b. large range/15– 40% range (in mothers below 18.5 BMI);
c. many/6 regions in the range of 20–30 % / many/5 regions in the range of 22–25 % (are below 18.5 BMI);
d. lowest in Addis and highest in Affar/Gambela;
a. hypothesis not supported; (do not award if unqualified)
b. no clear relationship / as malnutrition (mothers below 18.5 BMI) increases, there is no clear change in percentage male offspring;
c. however, male birth percentage is usually higher than female (above 50 %) regardless of BMI / 9 of the regions are above/2 regions are below;
a. no data about sex of the mothers’ other children;
b. BMI below 18.5 means individual is underweight but not necessarily malnourished;
c. the number of mothers sampled in each region is not known;
d. no comparison between town and country;
e. no information about age of mothers;
food shortages / famine / insufficient food / poor food quality / warfare / epidemics / poverty
| Date | May 2011 | Marks available | 1 | Reference code | 11M.3.SL.TZ1.1 |
| Level | Standard level | Paper | Paper 3 | Time zone | Time zone 1 |
| Command term | State | Question number | 1 | Adapted from | N/A |
Question
Vitamin C is an important component of a healthy diet. Because it is water-soluble it cannot be effectively stored and excess vitamin C is released in the urine. In order to investigate the ability of the body to retain different chemical forms of vitamin C, 17 healthy, female university students, between the ages of 18 and 22, were placed on a low vitamin C diet (< 5 mg per day) for three days. The test subjects were divided into two groups and were given an oral vitamin C loading of either ascorbic acid (176 mg) or dehydroascorbic acid (174 mg). Levels of vitamin C in the urine were measured six hours before and at regular intervals over a 24 hour period following vitamin C loading. The negative value indicates time before vitamin C loading.
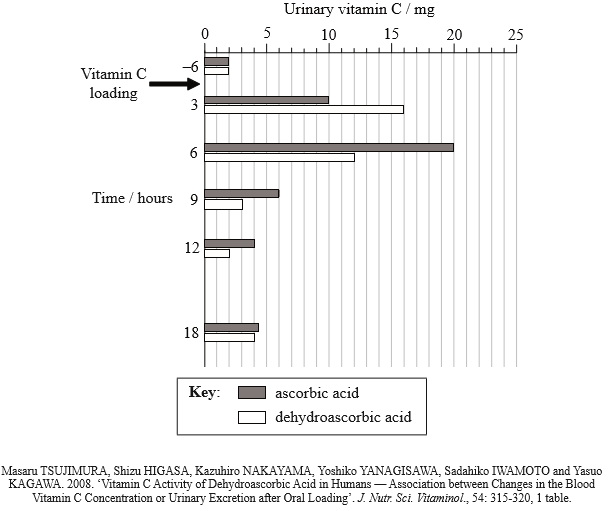
State the urinary vitamin C content for each of the two study groups six hours before vitamin C loading.
Ascorbic acid: ………………………………………………………………………………
Dehyrdoascorbic acid: …………………………………………………………………..
Calculate the percentage increase in urine levels of vitamin C for the ascorbic acid study group during the first three hours after vitamin C loading.
Compare the trends in vitamin C release for the two test groups during the first twelve hours after vitamin C loading.
Large individual differences in the urine level of ascorbic acid and dehydroascorbic acid were recorded between test subjects after 24 hours. Suggest one possible reason for these large individual differences.
Scurvy is a disease that is due to vitamin C deficiency. Evaluate the importance of this investigation for finding ways to combat vitamin C deficiency.
Markscheme
Ascorbic acid: 2 mg (units are needed)
Dehydroascorbic acid: 2 mg (units are needed)
Both required for the mark.
400 (%) (working not required)
more ascorbic acid (40 mg) than dehydroascorbic acid (33 mg) is released/excreted;
more dehydroascorbic acid (16 mg) than ascorbic acid (10 mg) is released/excreted in the first three hours / dehydroascorbic acid peaks before ascorbic acid;
from six hours onwards more ascorbic acid is released than dehydroascorbic acid;
maximum release of dehydroascorbic acid at three hours whereas maximum release of ascorbic acid at six hours;
ascorbic acid release rises then falls whereas dehydroascorbic release falls (until 12 hours after loading);
genetic variability / differences in vitamin C metabolism / differences in vitamin C requirements / differences in levels of uptake into blood / size/weight of individuals
both chemical forms are released/excreted so supplements need to be given regularly;
using dehydroascorbic acid instead of ascorbic acid does not improve vitamin C retention / dehydroascorbic acid could be marginally better as less is excreted;
study only looks at young/healthy/female subjects;
period of vitamin C deficiency is too short / need a longer period to allow scurvy to develop;
| Date | May 2011 | Marks available | 1 | Reference code | 11M.3.SL.TZ2.1 |
| Level | Standard level | Paper | Paper 3 | Time zone | Time zone 2 |
| Command term | Identify | Question number | 1 | Adapted from | N/A |
Question
In Australia, a study was undertaken among women to determine the vitamin D levels in their blood. Levels of vitamin D were categorized as sufficient, insufficient and deficient to determine how prevalent each category was. Three locations at three different latitudes and four different seasons were used. A data summary is shown in the graphs below.
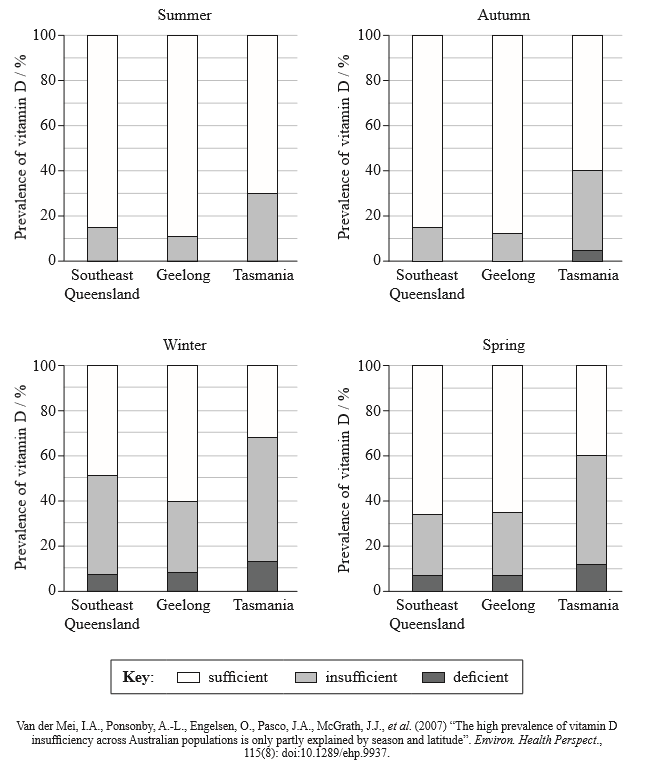
Identify the season when the women are least likely to suffer from vitamin D deficiency.
Using the data from all four seasons, identify the two locations where the patterns of vitamin D are most similar.
Determine what percentage of women in Geelong have insufficient vitamin D levels in winter.
Compare the deficiency levels of vitamin D at all three locations.
Location and season were found to account for only a small part of the deficiencies. Suggest, with reasons, how the behaviours of different people could influence the levels of vitamin D in their blood.
Markscheme
summer
Geelong and (Southeast) Queensland (both needed)
(40 −8) = 32% (accept answers in the range of 31 % to 33 %)
similarity:
none of the locations are deficient in Summer;
Geelong and (Southeast) Queensland have similar prevalence/levels of deficiency at all times of the year;
difference:
only Tasmania shows a deficiency in autumn;
Tasmania shows the highest prevalence of deficiency;
(Southeast) Queensland shows less prevalence/levels of deficiency overall;
To award [3], answers must address at least one similarity and one difference.
diets rich in vitamin D could raise vitamin D levels; (vice versa)
use of sunscreen/staying out of the sun/hats/clothing can reduce the production of vitamin D by the skin; (vice versa)
use of dietary supplements containing vitamin D can reduce deficiency levels;
| Date | May 2012 | Marks available | 1 | Reference code | 12M.3.SL.TZ1.1 |
| Level | Standard level | Paper | Paper 3 | Time zone | Time zone 1 |
| Command term | Identify | Question number | 1 | Adapted from | N/A |
Question
Iron, folic acid and vitamin B12 (cyanocobalamin) are important components of a healthy diet. These nutrients are necessary for the production of the red blood cells in the body that transport oxygen to the tissues. Deficiency of any of these nutrients can lead to anemia, a condition that causes weakness, tiredness and shortness of breath.
In a study of the Piaroa, a population living in a remote area of Venezuela, investigators discovered very high levels of anemia, especially amongst young children and females of childbearing age. The table below shows the incidence of anemia and deficiencies of iron, folic acid and vitamin B12 in this population, as a percentage.
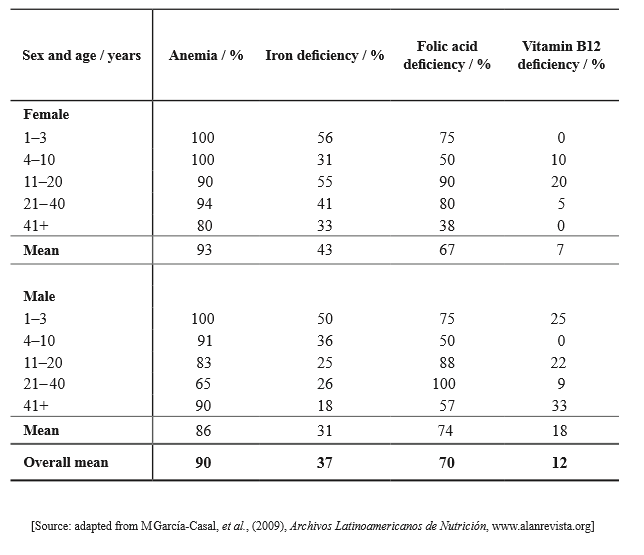
Identify the nutrient that is least likely to be deficient in a 45-year-old male in the Piaroa population.
Identify the age and sex of the group that suffers from the least amount of anemia in the Piaroa population.
Compare the data for the three nutrients in 11–20-year-old females with the data for 11–20-year-old males.
The data in the table indicates differences in the incidence of anemia between males and females. Suggest possible causes of these differences.
Markscheme
iron
21– 40-year-old males
more females than males have iron deficiency (55 %/25 %);
very small difference / 2 % difference between males and females for vitamin B12 deficiency and folic acid deficiency;
Allow valid numerical comparisons.
Accept reverse argument for first point.
females lose blood while menstruating;
extra nutrients needed while pregnant;
extra nutrients needed while breastfeeding;
differences in diet/vegetarian/vegan / low ferretin levels;
males receive more food than females/perceived to have greater need/status;
| Date | May 2010 | Marks available | 1 | Reference code | 10M.3.SL.TZ2.1 |
| Level | Standard level | Paper | Paper 3 | Time zone | Time zone 2 |
| Command term | Determine | Question number | 1 | Adapted from | N/A |
Question
Body mass index (BMI) is an important indicator of health. The relationship between a high BMI and percentage risk of developing type II diabetes was studied and the following data presented.
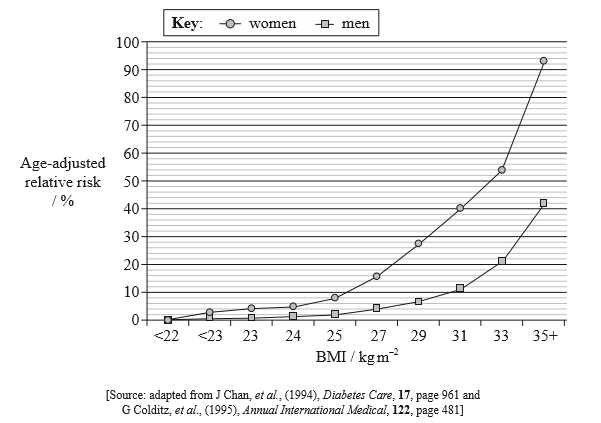
Describe the effect of increased BMI on the risk of developing type II diabetes.
Identify the risk of developing type II diabetes in men with a BMI of 33 kg m–2.
Determine, by indicating on the graph, the range of age-adjusted relative risk for women who are overweight but not obese.
Explain the dietary advice that should be given to a patient who has developed type II diabetes.
Markscheme
higher BMI increases risk of type II diabetes / risk increases as the BMI increases;
greater risk for women than for men / men have a lower risk than women;
values above 25 kg m-2 increase the risk of diabetes exponentially / BMI below 25 kg m-2 shows minimal risk;
21 % (allow answers in the range of 20 % to 22 %)
indicated by marks on the graph on the vertical axis or on the line of the woman 8 % to 33 % (allow 1 % error at either end)
Information must be indicated on the graph.
moderate portions of food to avoid fluctuations in blood sugar levels;
regular mealtimes to avoid fluctuations in blood sugar levels;
include unrefined carbohydrates because they are more slowly absorbed; (accept reverse for refined)
include carbohydrates with a low glycemic index; (accept reverse for high)
include fibre-rich foods to slow absorption of sugar;
limit saturated/trans fats/cholesterol because diabetes increases risk of coronary heart disease;
| Date | November 2011 | Marks available | 3 | Reference code | 11N.3.SL.TZ0.1 |
| Level | Standard level | Paper | Paper 3 | Time zone | TZ0 |
| Command term | Evaluate | Question number | 1 | Adapted from | N/A |
Question
Within a cross-sectional study “Fit for Life” in Germany, the body mass index (BMI) of volunteers aged between 16 and 25 years was investigated. Volunteers were also interviewed about their daily exercise habits. The graphs below show the percentage of men and women who were overweight, and the percentage who exercised daily.
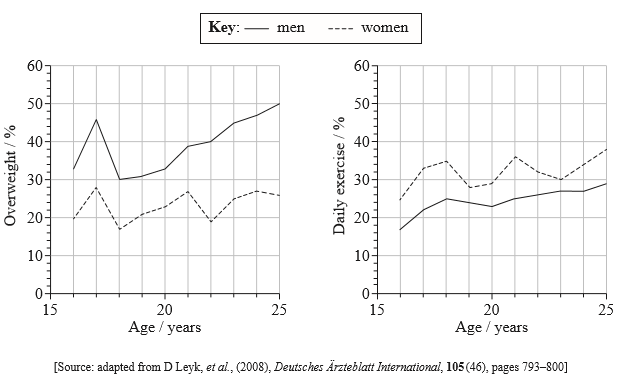
Measure the difference between the percentage of overweight men and the percentage of overweight women at age 20.
State the range of the body mass index (BMI) that corresponds to overweight status.
Compare the percentage of men and women who exercised daily.
Evaluate the hypothesis that being overweight is due to lack of exercise.
Markscheme
10 (%) (allow responses in the range of 9 to 11 %)
25.0 −29.9 / above 25 and below 30
Do not accept 30 as this is classed as obese.
more women exercise than men;
both show an increase (between ages 16 to 25);
similar trend lines over time / slightly greater increase in women;
women have greater increases and decreases/greater variability while men gradually increase/stays level;
Award any one of the above marking points if shown as a valid numerical comparison.
(hypothesis is supported) as the greater percentage of men are overweight and they exercise less than women / vice versa;
(hypothesis is supported) lowest percentages of overweight ages (18 and 20) correspond with peaks of exercise;
(hypothesis is not supported) as even though both men and women exercise more over time the percentage overweight also increases;
(hypothesis is not supported) other named factor which influences being overweight; (e.g. availability of cheap high energy foods / large portion sizes / increasing use of vehicles for transport / changes from active to sedentary occupations / genetics)
BMI does not consider muscle mass/bone structure/bone density;
only narrow range of ages considered;
| Date | November 2011 | Marks available | 3 | Reference code | 11N.3.SL.TZ0.2 |
| Level | Standard level | Paper | Paper 3 | Time zone | TZ0 |
| Command term | Outline | Question number | 2 | Adapted from | N/A |
Question
The following nutrients are listed on a packet of dry roasted peanuts.
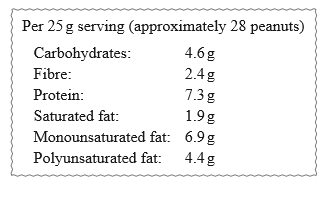
State which listed nutrient does not supply energy.
Deduce, with a reason, which listed nutrient provides the most energy per 25 g serving.
Outline the differences in molecular structure between the types of fat found in the peanuts.
Markscheme
fibre
monounsaturated fat;
fats contain more energy than carbohydrates or proteins;
fats contain 4000 kJ per 100 g/9 kcal per 100 g;
more monounsaturated fat present than other fats;
saturated and unsaturated fats differ in number of single and double carboncarbon bonds/ratio of hydrogen to carbon atoms in fatty acid chains;
saturated fat – carbon atoms all joined by single bonds / have no double bonds / have no increase in number of hydrogen atoms possible;
monounsaturated fat – one double bond in carbon chain / could add two hydrogens in the carbon chain;
polyunsaturated fat – two/more double bonds in the carbon chain;
saturated fatty acid chains tend to be straight while mono/polyunsaturated have kinks/bends;
| Date | November 2010 | Marks available | 2 | Reference code | 10N.3.SL.TZ0.1 |
| Level | Standard level | Paper | Paper 3 | Time zone | TZ0 |
| Command term | Compare | Question number | 1 | Adapted from | N/A |
Question
Rickets, caused by a defective vitamin D receptor (VDR), can be prevented by high calcium intake. A series of experiments were performed to test this. The results are shown in the graphs. Graph A shows the change in blood calcium levels after calcium administration in normal mice with and without addition of vitamin D. It also shows the change in blood calcium levels in mutant mice, which lack the vitamin D receptor. Graph B shows the change in blood calcium levels after calcium administration in normal mice after being subjected to one week of low, medium and high calcium diets.
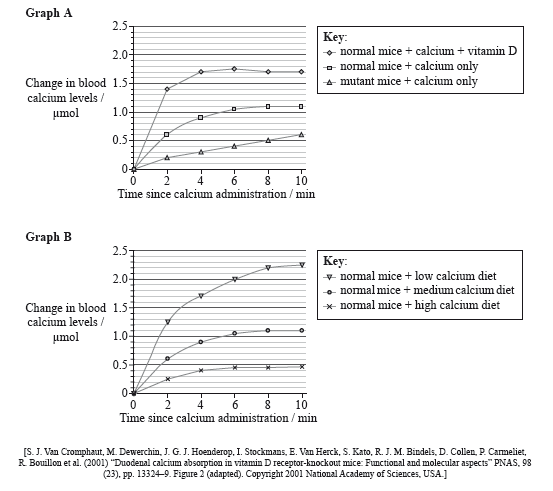
State the change in blood calcium levels in normal mice 10 minutes after the administration of calcium, with and without the addition of vitamin D.
With vitamin D:
Without vitamin D:
Compare the changes in blood calcium levels in normal mice and in mutant mice after the administration of calcium.
Explain, using graph B, the changes in blood calcium levels for the mice with different diets.
Discuss whether the scientists were able to support their hypothesis that rickets caused by the defective vitamin D receptor can be prevented by the intake of large amounts of calcium.
Markscheme
with vitamin D: (from 0.0 to) 1.7 μmol (units required – allow answers in the range of 1.65 to 1.75 μmol)
without vitamin D: (from 0.0 to) 1.1 μmol (units required – allow answers in the range of 1.05 to 1.15 μmol)
Both needed to award the mark.
a. both increase with time;
b. normal mice have a greater increase in blood calcium levels than mutant mice (after ten minutes);
c. normal mice have a maximum change of 1.1 μmol while mutant mice have a maximum change of 0.6 μmol;
d. mutant mice show gradual increase while normal mice show rapid increase followed by a plateau;
a. mice with low calcium diets have a greater increase in blood calcium levels (after calcium administration) because their body absorbs more calcium;
b. if they have had a high calcium diet they do not need to absorb so much calcium / vice versa;
c. probably receptors are all occupied/inhibited / less receptors;
a. hypothesis supported as blood calcium levels increased in mutant mice after intake of calcium (graph A);
b. but less than in normal mice / perhaps not enough to cure disease/rickets;
c. administering vitamin D also shows an increase in blood calcium levels (graph A);
d. but no good administering vitamin D as the receptor is defective;
e. in a high calcium diet, less absorption occurs (graph B), so might not be the solution;
f. should have tested mutant mice with different diets;
| Date | November 2009 | Marks available | 2 | Reference code | 09N.3.SL.TZ0.1 |
| Level | Standard level | Paper | Paper 3 | Time zone | TZ0 |
| Command term | Compare | Question number | 1 | Adapted from | N/A |
Question
Zinc (Zn) is an important dietary nutrient. More than 200 enzymes that are dependent on zinc have been identified. One consequence of zinc deficiency is suppression of appetite, due to reduced sensitivity to tastes and smells. A recent study compared the presence of zinc in tissue and fluid samples collected from 15 patients with anorexia nervosa to that from 15 control patients. The results are shown in the graphs below.
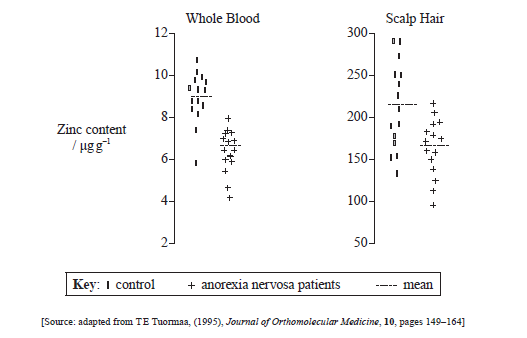
Compare the zinc content of scalp hair of the control group with that of the anorexia nervosa group.
Discuss whether whole blood zinc content of 6 μg g–1 would indicate that a person has anorexia nervosa.
Discuss whether dietary zinc supplementation would be an effective treatment for anorexia nervosa.
Zinc is a mineral. Distinguish between a mineral and a vitamin.
State the body mass index (BMI) below which a person is considered to be underweight.
Markscheme
mean zinc content higher in control group;
control group more variable;
overlap between two groups / highest of anorexia nervosa group equals mean of control group;
(data suggest this is) probable / could be symptom;
other conditions could lead to low zinc;
6 μg g–1 is within the lower range of “normal”;
zinc supplementation is necessary for insufficient dietary intake / improvement in below normal intake would be resolved;
improved appetite may result;
low zinc may be effect not cause of anorexia nervosa / other causes of anorexia;
minerals are inorganic while vitamins are organic;
minerals tend to be in ionic elemental form/small molecules while vitamins tend to be larger molecules;
(below a BMI of) 18.5kg m-2 (units needed)