▶️ Answer/Explanation
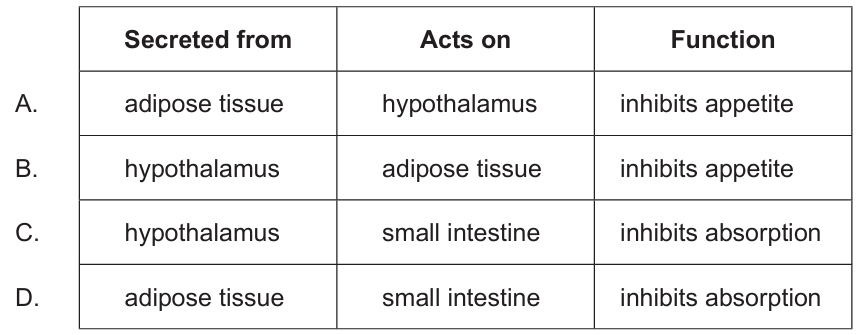
Answer: A
Leptin is produced by adipose (fat) tissue and signals fat storage levels to the brain. It acts on the hypothalamus to suppress appetite and regulate energy balance. The other options incorrectly describe either the source, target, or function of leptin.