Evaluating Study Design for Health Risk Factors
🌱 Key Concept
To assess how well a study is designed to determine health risk factors, focusing on:
- Sample selection
- Sample size
- Validity and reliability of data
1. Sample Selection
- Representative sample: Must reflect the population being studied.
Example: studying smoking habits → sample should include all age groups, genders, regions. - Random sampling: Reduces bias; each individual has an equal chance of selection.
- Stratified sampling: Ensures specific groups (age, gender, socioeconomic status) are represented.
- Tip: Poor sample selection → biased results → invalid conclusions.
2. Sample Size
- Larger sample size = more reliable and valid results.
- Small sample size → higher chance of random error, may not reflect the population.
- Balance feasibility vs accuracy: large enough to detect trends, small enough to be practical.
3. Validity of Data
- Internal validity: Study measures what it intends to measure.
Example: measuring effect of diet on heart disease → must accurately record diet and health outcomes. - External validity: Results can be generalised to the wider population.
4. Reliability of Data
- Consistency: Repeating the study under the same conditions should give similar results.
- Standardised methods: Same measurement tools, procedures, and definitions.
- Minimising errors: Training observers, calibrating equipment.
5. Other Considerations
- Control for confounding variables: Other factors that can affect results (e.g., genetics, lifestyle).
- Ethical considerations: Consent, confidentiality, minimal risk.
- Study type matters: Observational vs experimental studies affect reliability of conclusions.
🧠 Quick Recap
Sample Selection: Must be representative; random or stratified
Sample Size: Larger = more reliable; balance feasibility
Validity: Measures what it intends; results generalisable
Reliability: Consistent results; standardised methods
Confounding Factors: Must be controlled to avoid misleading conclusions
Blood Cholesterol, Lipoproteins & Cardiovascular Disease (CVD)
🌱 Key Concepts
Cholesterol levels in the blood are important indicators of heart health. Understanding HDLs, LDLs, and total cholesterol helps assess the risk of CVD.
1. Blood Cholesterol
- Cholesterol: a lipid essential for cell membranes and hormone production.
- Normal range: ~<200 mg/dL total cholesterol in adults.
- Too much cholesterol can lead to plaque formation in arteries → atherosclerosis → heart disease.
2. Lipoproteins
Cholesterol is transported in blood by lipoproteins:
| Type | Role | Health Significance |
|---|---|---|
| HDL (High-Density Lipoprotein) | “Good cholesterol” – carries cholesterol from tissues to liver for disposal | High HDL → protective, lowers CVD risk |
| LDL (Low-Density Lipoprotein) | “Bad cholesterol” – carries cholesterol from liver to tissues | High LDL → increases risk of plaque formation → CVD |
3. Analysing Data on Cholesterol & Health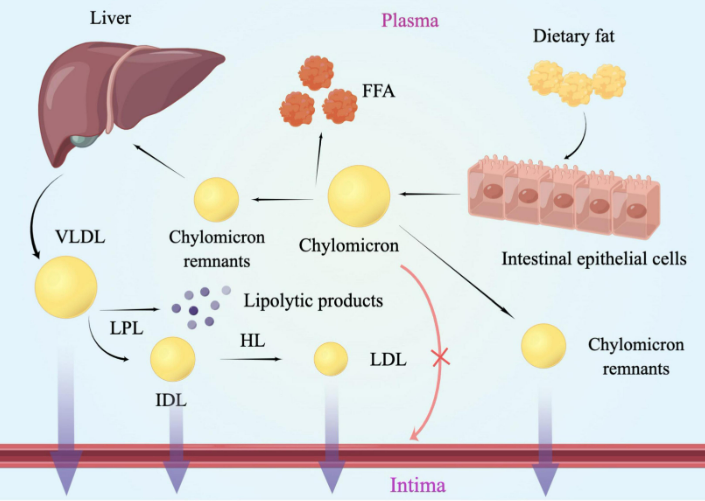
- Compare total cholesterol, LDL, HDL levels with CVD incidence.
- Look for trends: e.g., high LDL + low HDL → higher risk of heart disease.
- Semi-quantitative studies: epidemiological surveys, cohort studies.
4. Evidence for Causal Relationship
- Population studies: Countries/regions with high average LDL cholesterol → higher rates of CVD.
- Intervention studies: Reducing LDL (through diet or drugs) → decreases incidence of heart attacks.
- Genetic evidence: People with familial hypercholesterolemia (high LDL from birth) → very high CVD risk.
Conclusion:
- High LDL and total cholesterol levels are causally linked to CVD.
- High HDL is protective.
🧠 Quick Recap
LDL = bad, HDL = good.
High LDL & total cholesterol → ↑ CVD risk.
Low HDL → ↑ CVD risk.
Reducing LDL or increasing HDL improves heart health.