Topic 6.4: gas exchange

This unit will last 3 school days
Essential idea:
- The lungs are actively ventilated to ensure that gas exchange can occur passively.
Nature of science:
- Obtain evidence for theories—epidemiological studies have contributed to our understanding of the causes of lung cancer. (1.8)
- Define epidemiology.
- Outline how epidemiological studies contributed to understanding the association between smoking and lung cancer.
The processes involved in physiological respiration are:
- Ventilation: The exchange of air between the atmosphere and the lungs – achieved by the physical act of breathing
- Gas Exchange: The exchange of oxygen and carbon dioxide between the alveoli and bloodstream (via passive diffusion)
- Cell Respiration: The release of energy (ATP) from organic molecules – it is enhanced by the presence of oxygen (aerobic)
Physiological respiration involves the transport of oxygen to cells within the tissues, where energy production occurs
- Small single celled organisms can easily diffuse gas in and out of the cell as long as they are in an environment where concentration gradients exist for passive diffusion. For example, O2 in water can diffuse into a protist as long as the concentration of oxygen in the surrounding water is greater than the oxygen levels inside the protist cell.
- Human bodies are surrounded and protected by layers of skin. Thecells in the tissue that need oxygen for respiration are too far away, too protected, and too numerous to allow direct diffusion with their environment.
- Humans need a system to keep a fresh supply of O2 and to get rid of excess CO2.
- The ventilation system provides a fresh supply of O2 in the alveoli, allowing the oxygen to diffuse into the blood capillaries surrounding them
- The oxygen is then transported to all the tissues in the body.
- The CO2 in the tissues is transported by the blood to the lungs, where it diffuses into the alveoli and is exhaled into the surrounding atmosphere.
- Fresh supplies of O2 also makes sure that a steep concentration gradient exists where gas is exchanged to allow efficient exchange of O2
- The blood arriving at the alveoli via the pulmonary arteries, arterioles and then capillaries, is rich in CO2, thus creating a concentration gradient between the capillaries and the alveoli, allowing CO2 to rapidly diffuse out of the blood in the capillaries into the alveoli
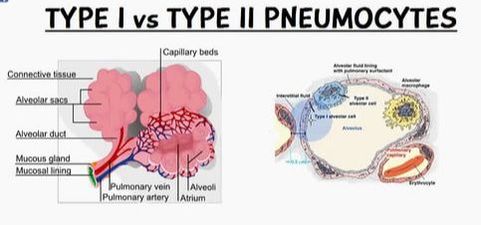
Pneumocytes (or alveolar cells) are the cells that line the alveoli and comprise of the majority of the inner surface of the lungs
- The walls of the alveoli are predominately made from a single layer of epithelial cells called Type I pneumocytes
- They are squamous (flattened) in shape and extremely thin (~ 0.15µm) – minimising diffusion distance for respiratory gases
- Since the alveoli are surrounded by capillaries that are also only one cell thick, oxygen and carbon dioxide have a very short distance to diffuse into the blood from the alveoli and out of the blood into the alveoli respectively
- This adaptation allows for a rapid rate of gas exchange
- Connected by occluding junctions, which prevents the leakage of tissue fluid into the alveolar air space
- Amitotic and unable to replicate, however type II cells can differentiate into type I cells if required.
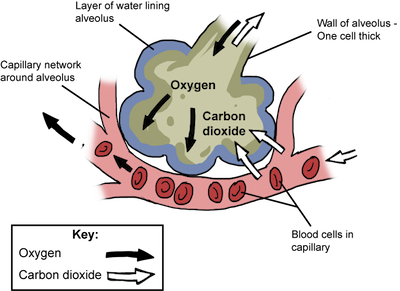
Alveoli are lined by a layer of liquid in order to create a moist surface conducive to gas exchange with the capillaries
- It is easier for oxygen to diffuse across the alveolar and capillary membranes when dissolved in liquid
- About 5% of the inner surface of the alveoli consists of Type II pneumocytes
- These cells secrete a liquid made of proteins and lipids called surfactant
- This liquid allows oxygen to dissolve into the surfactant and then diffuse into the blood
- It also provides a medium for carbon dioxide to evaporate into the air inside the alveoli in order to be exhaled
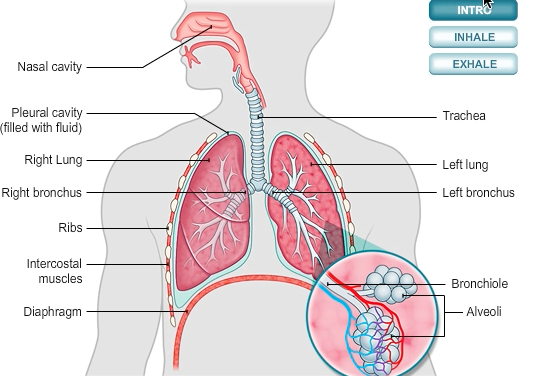
- Air enters the respiratory system through the nose or mouth and travels through the pharynx and then the trachea (made from rings of cartilage)
- The trachea divides into two bronchi (left and right)
- Inside each lung the bronchi divide into many smaller tubes called bronchioles
- These numerous bronchioles form a tree root-like structure that spreads throughout the lungs
- Each bronchiole ends in a cluster of air sacs called alveoli
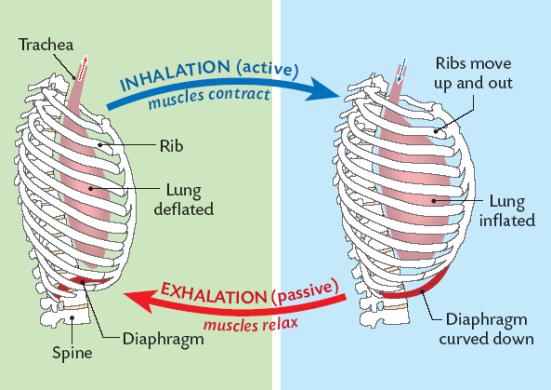
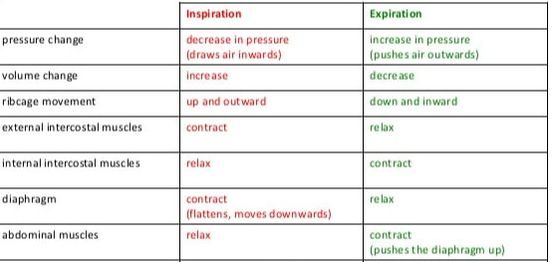
Breathing is the active movement of respiratory muscles that enables the passage of air into and out of the lungs. The contraction of respiratory muscles changes the volume of the thoracic cavity (i.e. the chest).
When the pressure in the chest is less than the atmospheric pressure, air will move into the lungs (inspiration)
When the pressure in the chest is greater than the atmospheric pressure, air will move out of the lungs (expiration
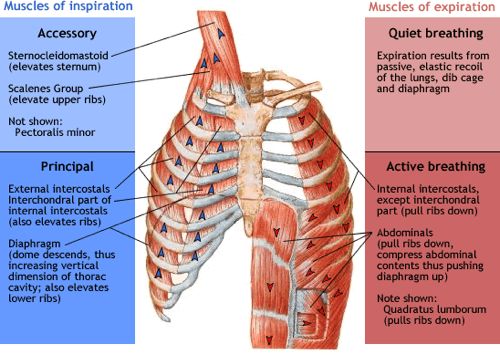
Inspiration (inhaling) and expiration (exhaling) are controlled by two sets of antagonistic muscle groups. When different muscles work together to perform opposite movements, they do so in an antagonistic fashion; when one muscle contracts the other will relax
- When muscles contract and shorten (do work), they exert a pulling force that causes movement
- The antagonistic muscle will relax and lengthen because of the pulling force of the other muscle; therefore no work is done
- For example, when one breaths in air, the external intercostal muscles contract, moving the ribcage up and out and the internal intercostal muscles relax (biceps and triceps work in similar fashion in our arms). The opposite occurs during expiration.
- Muscles therefore only cause movement in one direction while contracting (antagonistic pair relaxes). Movement in the other direction occurs when the other muscle of the pair contracts and the first muscle relaxes
Lung cancer describes the uncontrolled proliferation of lung cells, leading to the abnormal growth of lung tissue (tumour). The abnormal growth can impact on normal tissue function, leading to a variety of symptoms according to size and location. The tumours can remain in place (benign) or spread to other regions of the body (malignant)
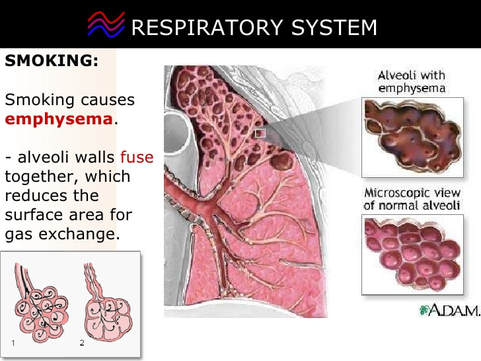
Smoking
- is the number one cause of lung cancer
- there is an extremely high correlation with the number of cigarettes an individual smokes in a day and the incidence of lung cancer
- Cigarettes contain a high number of carcinogens, such as polycyclic aromatic hydrocarbons and nitrosamines
- Second-hand smoke can also be considered a cause of cancer in non-smokers
Air Pollution
- Air pollution from exhaust fumes containing nitrogen oxides, fumes from diesel engines and smoke from burning carbon compounds such as coal are a minor cause of lung cancer. This depends on where in the world you live and the air quality.
Radon Gas
- In some parts of the world, this radioactive gas can leak out of certain rocks such as granite, accumulating in poorly ventilated buildings
Asbestos
Construction sites, factories and mines can have dust particles in the air. If steps aren’t taken to properly protect the worker’s, lung cancers can develop.
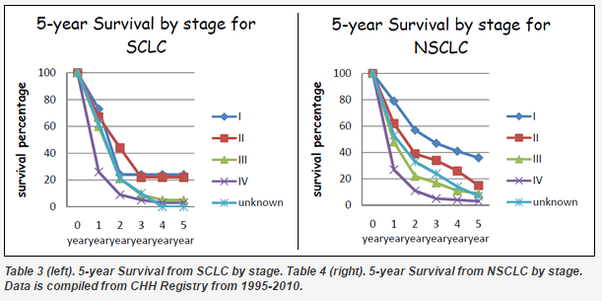
Lung cancer is a very serious disease and the consequences can be severe, especially if the cancer is not recognized early on.
- If the tumour is large when it is discovered, metastasis might have occurred (cancer spreads to other parts of the body and forms secondary tumours). In these cases, mortality rates are very high. If the tumour is found early on, parts of the affected lung with the tumour can be removed and chemotherapy can be used to help kill the rest of the cancer cells. Re-occurrence of the disease is quite common.
6.4.A2 Causes and consequences of emphysema.
- Outline the causes of lung cancer.
- List symptoms of lung cancer.
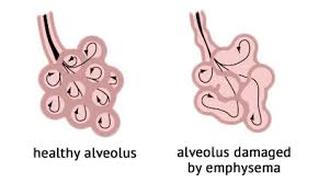
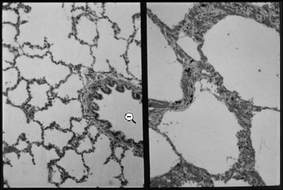
Emphysema is a lung condition whereby the walls of the alveoli lose their elasticity due to damage to the alveolar walls
- Emphysema is another respiratory disease that is often linked to smoking
- The loss of elasticity results in the abnormal enlargement of the alveoli, leading to a lower total surface area for gas exchange
- The degradation of the alveolar walls can cause holes to develop and alveoli to merge into huge air spaces (pulmona
- Phagocytes (white blood cells that engulf foreign bacteria) usually prevent lung infections and produce a hydrolytic enzyme called elastase
- An enzyme inhibitor usually prevents elastase from digesting lung tissue
- Smokers lungs generally contain a high number of these phagocytes/macrophages in their blood
- Since there is a higher level of phagocytes, more elastase is produced;however, not enough of the inhibitor that prevents elastase from digesting lung tissue
- This results in the destruction of elastic fibres of the alveolar walls by the enzyme elastase
- The alveoli can become over-inflated and fail to recoil properly
- Small holes can also develop in the walls of the alveoli
- The alveoli can merge forming huge air spaces and a lower surface area.
- This destruction cannot be reversed
 |  |  |
Ventilation consists of inhalation (inspiration) and exhalation (expiration)
Inhalation
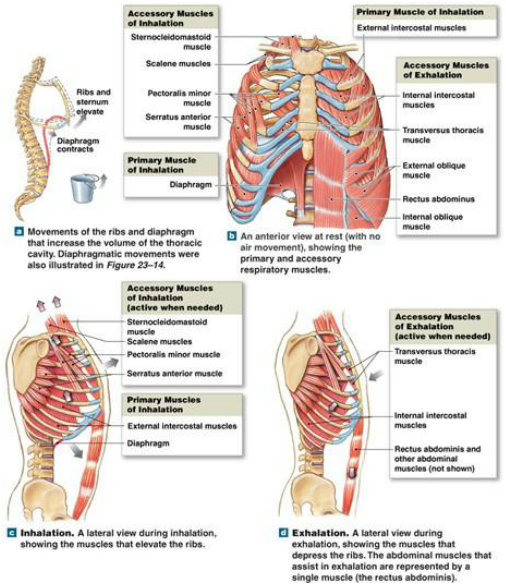
- External intercostal muscles contract pulling the ribs upwards and outwards.
- The diaphragm which is a flat sheet of muscle extending across the bottom of the rib cage contracts and flattens out.
- These two actions enlarge the thoracic cavity surrounded the lungs, thereby increasing the volume of the lungs.
- When the volume of the lungs increases, the pressure inside the lungs decreases and becomes lower than the pressure in the surrounding atmosphere.
- Since gas moves from higher pressure to lower pressure, air rushes into the lungs from the surrounding atmosphere to equalize the pressure.
Exhalation
- The external intercostal muscles relax and the diaphragm snaps back to its original shape (domed shape).
- This moves the ribs back down and inwards and decreases the volume of the thoracic cavity and the lungs.
- This decrease in volume increases the pressure inside the lungs.
- Since the pressure inside the lungs is now greater than the atmospheric pressure, and gas moves from high pressure to low pressure, air rushes out of the lungs into the surrounding environment.
- NOTE: If there is a forced exhalation (push and squeeze the air out of the lungs) the internal intercostal muscles will also contract along with the abdominal muscles to pull the rib cage down and squeeze the organs in the abdomen
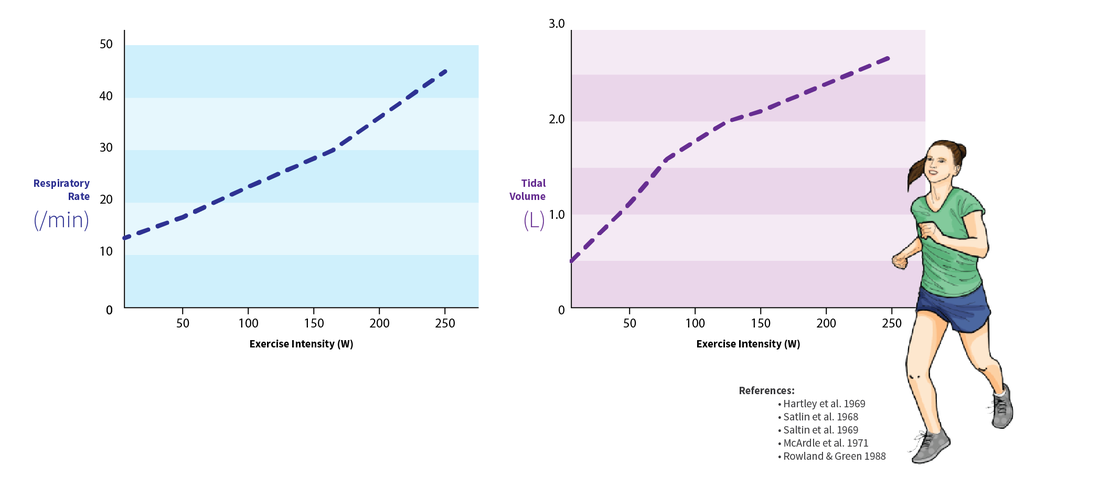
Ventilation in humans changes in response to levels of physical activity, as the body’s energy demands are increased
- ATP production (via cellular respiration) produces carbon dioxide as a waste product (and may consume oxygen aerobically)
- Changes in blood CO2 levels are detected by chemosensors in the walls of the arteries which send signals to the brainstem
- As exercise intensity increases, so does the demand for gas exchange, leading to an increase in levels of ventilation
Exercise will influence ventilation in two main ways:
- Increase ventilation rate (a greater frequency of breaths allows for a more continuous exchange of gases)
- Increase tidal volume (increasing the volume of air taken in and out per breath allows for more air in the lungs to be exchanged
Breathing and Exchange of Gases
Table of Content
- What is Breathing and Respiration?
- Respiratory organs
- Human Respiratory System
- Mechanism of Breathing
- Respiratory volumes and capacities
- Exchange of gases
- Transport of gases
- Regulation of Respiration
What is Breathing and Respiration?
Breathing is the process of taking in oxygen and giving out carbon-dioxide. Respiration is a catabolic process of breakdown of energy rich molecules to produce energy needed for the survival of the organism.
Respiratory organs
Different organisms have different respiratory organs depending upon the habitat and level of organization.
Earthworm has moist skin that participates in respiration. This type of respiration is known as Cutaneous Respiration. Insects have tracheal tubes that are respiratory in function. Aquatic animals have gills as respiratory organs. Higher animals have lungs for respiration, including human beings.
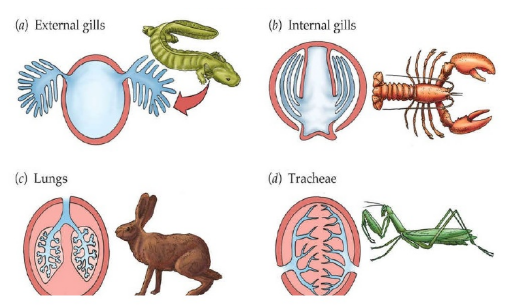
Fig. 1. Different respiratory organs
Human Respiratory System
Humans have a pair of nostrils which leads into the nasal passage. Nasal chamber then leads to pharynx which is common passage for food as well as air. The pharynx opens through the larynx region into the trachea. Larynx is a sound box which helps in sound production. During eating larynx is covered by a flap known as Epiglottis to prevent the entry of the food into the larynx. Trachea is straight tube that divides into left and right primary bronchi. Primary bronchi further divide into secondary and tertiary bronchi and bronchioles. Each terminal bronchioles give rise thin, vascularized bag-like structure known as Alveoli.
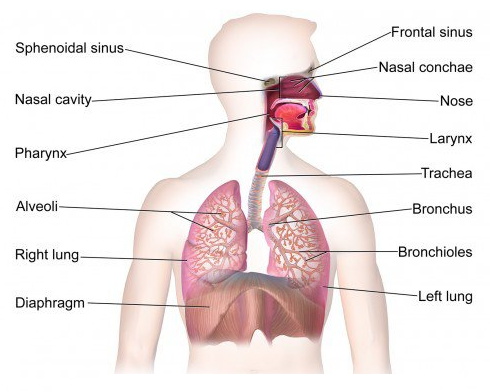
Fig. 2. Human respiratory system
Humans have pair of lungs that are covered by a membrane known as Pleural Membrane. Between the outer and the inner pleural membrane is pleural fluid that prevents friction on the lung surface.
Respiration involves following steps:
- Pulmonary ventilation which involves taking in atmospheric air and releasing carbon-dioxide rich air.
- Diffusion of oxygen and carbon-dioxide across the alveolar membrane.
- Transport of gases by the blood.
- Diffusion of O2 and CO2 between blood and tissues.
- Utilization of oxygen by the cells for catabolic reactions and release of carbon-dioxide.
Mechanism of Breathing
Breathing involves two processes- Inspiration and Expiration.
Inspiration:
- Process of taking atmospheric air in is known as Inspiration.
- It is an active process.
- Pressure inside the lungs is less than the atmospheric pressure.
- Contraction of diaphragm increases the volume of the thoracic cavity.
- External inter-coastal muscles also contract which raises the ribs to increase the volume of thoracic cavity.

Fig. 3. Mechanism of breathing
Expiration:
- Process of giving out carbon-dioxide is known as Expiration.
- It is a passive process.
- Pressure inside the lungs is more than the atmospheric pressure.
- Relaxation of diaphragm decreases the volume of the thoracic cavity.
- External inter-coastal muscles relax which lowers the ribs to decrease the volume of the thoracic cavity.
Respiratory volumes and capacities
Tidal Volume (TV) is the volume of air that is inspired or expired during normal respiration. It is approximately 500 ml for healthy person.
Inspiratory Reserve Volume (IRV) is the additional air a person can inspire after forceful inspiration. It is about 2500 ml to 3000 ml.
Expiratory Reserve Volume (ERV) is the additional air a person can expire after forceful expiration. It is about 1000 ml to 1100 ml.
Residual Volume (RV) is the volume of air left in the lungs after forceful expiration. It is about 1100 ml to 1200 ml.
Inspiratory Capacity (IC) is the volume of air a person can inspire after normal expiration. Tidal volume and inspiratory reserve volume together forms the inspiratory capacity.
Expiratory Capacity (EC) is the volume of air a person can expire after normal inspiration. Tidal volume and expiratory reserve volume forms the expiratory capacity.
Functional Residual Capacity (FRC) includes expiratory reserve volume and residual volume.
Vital Capacity is the volume of air a person can breathe after forceful expiration.
Total lung capacity includes RV, ERV, TV and IRV.
Exchange of gases
Exchange of gases occurs in alveoli. Exchange of gases occurs by diffusion based on pressure or concentration gradient. Two important parameters that affects the rate of diffusion are – solubility of gases and thickness of membrane.
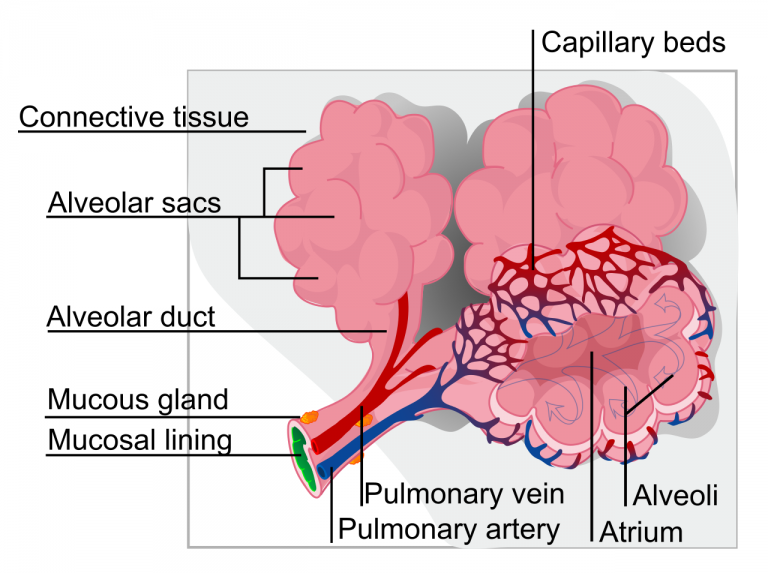
Fig. 4. Structure of alveoli
Pressure contributed by each gas in a mixture of gas is known as partial pressure. Partial pressure of oxygen and carbon-dioxide is represented by pO2 and pCO2 respectively.
The partial pressure of oxygen in alveoli is 104 mmHg whereas in blood is 40 mmHg. Similarly, the partial pressure of carbon-dioxide is 40 mmHg in alveoli and 45 mmHg in blood. This creates a concentration gradient between the blood and the alveoli. The diffusion membrane is made up of 3 layers – the thin squamous epithelium of alveoli, the endothelium of alveolar capillaries and the basement substance in between them.
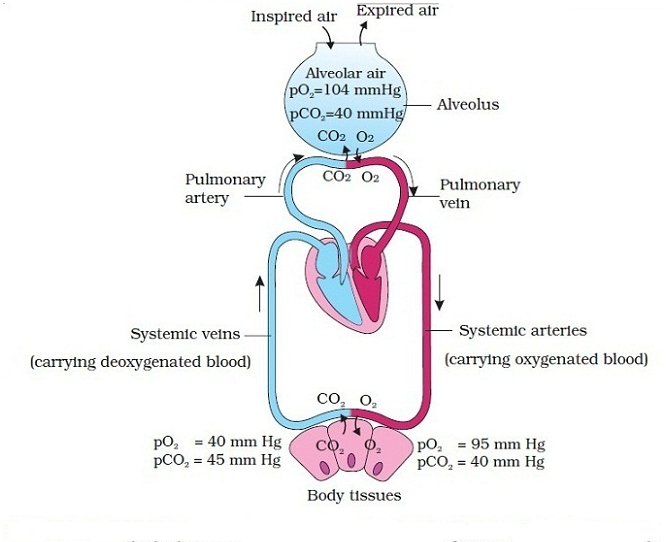
Fig. 5. Exchange of gases
Transport of gases/how oxygen and carbon-dioxide transported in blood?
The transport of oxygen and carbon-dioxide occurs via blood. About 97% of transport of oxygen occurs by blood. And remaining 3% is transported by plasma. Similarly, 70% of carbon-dioxide is transported in the form of bicarbonate. Around 25% is transported via red blood cells. Around 7% is transported in dissolved state via plasma.
Transport of oxygen
Red blood cells contain iron containing red colored pigment known as Hemoglobin. Hemoglobin binds oxygen in a reversible manner to form oxy-hemoglobin. Single hemoglobin molecule can bind 4 oxygen molecules. Partial pressure of oxygen determines the binding of oxygen with hemoglobin. When percent saturation of hemoglobin is plotted against partial pressure of oxygen, a sigmoid curve is obtained. This is known as Oxygen Dissociation curve. High partial pressure of oxygen, low partial pressure of carbon-dioxide, low temperature promotes oxy-hemoglobin formation whereas low partial pressure of oxygen, high partial pressure of carbon-dioxide in tissues promotes dissociation of oxygen from hemoglobin.
So, oxygen binds to hemoglobin in lungs and gets dissociated in tissues.
Transport of carbon-dioxide
About 20-25% of carbon-dioxide is transported in the form of carbamino-hemoglobin. This occurs when partial pressure of carbon-dioxide is high is tissues. The dissociation of carbon-dioxide from hemoglobin occurs in alveoli where partial pressure of carbon-dioxide is low. Red blood cells contain a very important enzyme known as Carbonic Anhydrase. The following reactions occurs in presence of carbonic anhydrase:
![]()
Fig. 6. Transport of carbon-dioxide
Regulation of Respiration
Neural system regulates the respiration. Respiratory control is located in medulla region of the brain. Another center that controls the respiration is known as Pneumotaxic center located in pons.
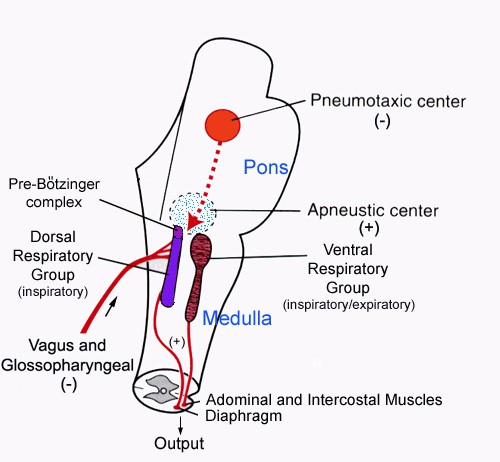
Fig. 7. Regulation of respiration